transplantation re-thought:
invisible organs instead of lifelong immunosuppression.
Subproject 1 - Ex vivo Organ Modification
Genetic ex vivo organ modification is used to modify transplants such that they can no longer be rejected.
Transplantation re-thought: invisible organs instead of lifelong immunosuppression.
„Transplantation needs to be re-thought in order to break new ground. Invisible organs offer the prospect for a life without rejection and immunosuppression, better graft survival, better quality of life and more available organs.“

Our Vision
Rejection and organ shortage are the major hurdles in transplantation medicine. Therefore, the wishful thinking is still the creation of tolerance towards indefinitely available organs. At least when it comes to avoiding rejection, the progress is obvious. The basic idea, however, is almost always to modify the recipient's immune system to achieve immunological blindness to the transplanted organ. But even today the induction of a transplant-specific tolerance remains an unfulfilled dream.
Instead, immunological blindness has to be purchased by a general, usually lifelong, immunosuppression, which, despite all the progress made in biomarkers, immunosuppressive drugs and monitoring, still places a high burden on the patient. Our vision is a completely new approach to solving the problem of organ rejection: instead of inducing immunological blindness in the organ recipient, an immunological invisibility of the donor organ will be created – for a life without rejection and immunosuppression, better graft survival, better quality of life and more available organs.
Our Objectives
The aim of subproject 1 is to reduce the immunogenicity of donor organs by selectively and permanently switching off the tissue markers. As a result, the target structures for immunologically mediated rejection are missing, so that an organ can no longer be recognized as foreign. The findings of the innovation network are intended to provide the basis for a subsequent clinical study in order to enable the application in humans.
The immunogenicity of a transplant is determined by the gene products of the Major Histocompatibility Complex (MHC), which in humans are referred to as Human Leukocyte Antigens (HLA). The mechanism by which the immune system recognizes allogeneic cells as foreign is based on the recognition of these HLA-antigens on the cell surface by cytotoxic T-cells and antibodies. The HLA antigens are extremely polymorphic, so that thousands of variants exist which trigger organ rejection in case of a mismatched organ transplant. But even in the case of an extremely rare complete HLA match between donor and recipient, rejection occurs regularly because short peptides from all endogenous proteins are presented in the HLA molecules, which exhibit countless disparities between genetically distinct individuals and are referred to as minor histocompatibility antigens (mHag).
The concept of tissue marker deactivation is based on a genetic modification of the organs by viral transduction during ex vivo perfusion in an organ preservation system. The cells are genetically modified in such a way that the MHC genes can no longer be expressed as proteins on the cell surface. The elimination of these target structures of immunological rejection at the donor-recipient interface leads to immunological invisibility of the modified cells to the recipient's immune system. An immunological recognition as foreign is thus no longer possible despite a fully functional immune system of the recipient. In previous investigations with cells and tissues, rejection could be completely prevented in this way without the need for immunosuppression.
This project investigates ex vivo organ modification and transplantation of optimized organs in a preclinical kidney transplant model. The methods of ex vivo transduction will be developed and the optimal conditions for organ perfusion will be determined in cooperation with IKME/HsH. Once protocols have been established, modified kidneys are transplanted into allogeneic recipient pigs and rejection monitoring is performed. If the process is successful, the clinical study is prepared.
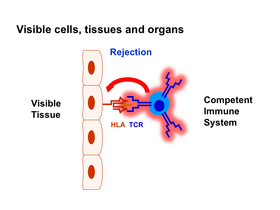
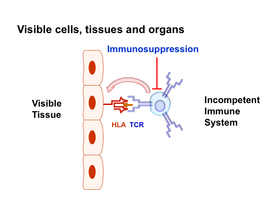
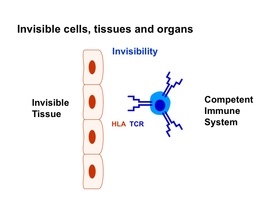
Figure legend:
Tissue markers are the target structures of T cells that cause rejection. Immunosuppression leads to the inactivation of these immune cells and the attenuation of rejection, but at the expense of a functioning immune system. By switching off the tissue markers, the immune cells can no longer recognize the transplant as foreign, it becomes invisible to them, so that the immune system of the recipient no longer needs to be weakened by immunosuppression.
Head Subproject 1
Professor Dr. Rainer Blasczyk
Institute of Transfusion Medicine and Transplant Engineering
Hannover Medical School
Carl-Neuberg-Str. 1
30625 Hanover, Germany
Phone: +49 (0) 511 532-6700

Professor Dr. Constanca Figueiredo
Institute of Transfusion Medicine and Transplant Engineering
Hannover Medical School
Carl-Neuberg-Str. 1
30625 Hanover, Germany
Phone: +49 (0) 511 532-9711

Staff Subproject 1
Dr. Chen Chen-Wacker
Dr. Olena Pogozhykh
Dr. Nadine Wenzel
Dr. Yuliia Yuzefovych
Marco Carvalho Oliveira
Franziska Hack
Emilio Valdivia
Tamina Rother
Susanne Aufderbeck
Beata Meyer
Yvonne Speidel